


1Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, 2National Center for Dual Diagnosis, Innlandet Hospital Trust, Brumundal, Norway, 3Department of Dermatology, Justus Liebig University, Giessen, Germany, 4Department of Psychology, University of Zaragoza, Zaragoza, Spain, 5Department of Public Health, Hedmark University College, Elverum, Norway, 6Department of Dermatology, ULB-Erasme Hospital, Brussels, Belgium, 7Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark, 8Department of Dermatology, University Hospital of Brest, Brest, France, 9Department of Dermatology, University of Szeged, Szeged, Hungary, 10Section of Biostatistics, University of Oslo, Oslo, Norway, 11Clinical Epidemiology Unit, Istituto Dermopatico dell’Immacolata, Rome, Italy, 12Health, Medical and Neuropsychology unit, Leiden University, Leiden, The Netherlands, 13Department of Dermatology, Institute of Clinical Medicine, Oslo University Hospital, University of Oslo, Oslo, 14Department of Dermatology, Stavanger University Hospital, Stavanger, Norway, 15Department of Clinical Derm-atology and Cosmetology, Moscow Scientific and Practical Center of Dermatovenereology and Cosmetology, Moscow, Russia, 16Department of Dermatology, Alcaniz Hospital, Alcaniz, Spain, 17Department of Dermatology, Sisli Etfal Teaching and Research Hospital, Istanbul, Turkey, 18Department of Dermatology, Cardiff University School of Medicine, Cardiff, 19School of Life and Medical Sciences, University of Hertfordshire, Hatfield, and Institute for Medicines Development, Cardiff, UK, and 20Institute of Medical Psychology, Justus Liebig University, Giessen, Germany
There are limited data on the differences in the impact of psoriasis between various countries with respect to quality of life (QoL). The aim of this study was to explore the psychosocial health of patients with psoriasis in different European countries. A total of 682 patients were recruited in 13 European countries. All patients completed a questionnaire regarding socio-demographic information, negative life events, suicidal ideation and satisfaction with their dermatologist. Depression and anxiety were assessed with the Hospital Anxiety and Depression Scale (HADS), and QoL with the Dermatology Life Quality Index (DLQI) and EuroQoL (EQ-5D). The lowest anxiety and depression scoring was noted in patients from Denmark, the lowest level of impairment in QoL in subjects from Spain, and the highest level of impairment in QoL in patients from Italy. The most relevant parameters influencing patients’ well-being were severity of pruritus and satisfaction with their dermatologist. The level of anxiety and depression symptoms correlated significantly with suicidal ideation.
Key words: psoriasis, quality of life, depression, anxiety, self-esteem.
Accepted Aug 9, 2017; Epub ahead of print Aug 10, 2017
Acta Derm Venereol 2017; 97: xx–xx.
Corr: Jacek Szepietowski, Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Cha?ubi?skiego 1, PL-50-368 Wroclaw, Poland. E-mail: jacek.szepietowski@umed.wroc.pl
Psoriasis is a common chronic inflammatory skin disorder with a substantial emotional impact on patients. Prevalence studies have shown uniformly high rates of psychopathology among people with psoriasis (1–4). For instance, anxiety symptoms were found much more commonly in patients with psoriasis compared with controls, with an adjusted odds ratio (OR) of 2.91 (95% confidence interval (95% CI) 2.01–4.21) for anxiety disorders in subjects with psoriasis (4). People with psoriasis were also more likely to be clinically depressed (1). Of note, psychological factors, such as stress, anxiety and depressed mood, may influence the course of the disease and, along with the impact of psoriatic symptoms, impair patients’ quality of life (QoL). Importantly, the impact of psoriasis on health-related QoL (HRQoL) seems to be as great as that of other major medical conditions, such as cancer, heart failure, diabetes and depression (3). Moreover, there was a significant association between having psoriasis and having suicidal thoughts: 67.6% of subjects with psoriasis reported suicidal ideation because of their skin problem (4). Depression in psoriasis might also be linked with higher cardiovascular morbidity and mortality, as it may play a role in promoting subclinical atherosclerosis beyond traditional cardiovascular risk factors. It was shown that depression might be associated with increased vascular inflammation and formation of coronary plaques (5, 6). Therefore, it could be recommended that patients with psoriasis should be systematically screened to identify clinically important levels of depression and anxiety that may be missed while assessing HRQoL alone (7).
It is not known whether depression level and other psychopathological symptoms in psoriasis correlate with disease severity, as current data are contradictory. Some authors have suggested that social stigmatization, high stress levels, physical limitations, depression, employment problems and other psychosocial co-morbidities experienced by patients with psoriasis are not always proportional to, or predicted by, other measurements of disease severity, such as body surface area involvement or plaque severity (2). However, other researchers report that the severity of psoriasis has a significant impact on the wellbeing of affected individuals, as the burden of overall medical comorbidities increases with disease severity in the psoriatic population, and severe psoriasis increases overall mortality, while mild psoriasis does not (8, 9). Therefore, although there may be discordance between severity of skin lesions and distress, severity of psoriasis may have some effect on rates of depression and suicidality (8).
The psychosocial health of psoriatic patients may be influenced not only by the disease itself, but also by other factors, such as patients’ economic status, occupation and family support. Also, wider factors, such as the healthcare system organization, access to different therapeutic options, or even climate may play a role (10, 11). However, despite the psychological aspects of psoriasis having been widely reported, there is little comparative information from different countries (12, 13). It is probable that patients with psoriasis from different regions may perceive their disease differently. In the present study we performed detailed analysis of data to identify differences among psoriatic patients from various countries, especially regarding determinants of psychosocial health deterioration, including HRQoL, anxiety and depression.
This study focused on the psoriatic patients participating in the project “The psychological burden of skin diseases: a cross-sectional multicenter study among dermatological outpatients in 13 European countries” run by the European Society of Dermatology and Psychiatry (ESDaP). In this observational, cross-sectional multicentre study, patients were recruited from dermatological outpatient clinics in 13 European countries from November 2011 to February 2013. At each study centre consecutive adult outpatients were invited to participate in the study on one or more random days, until 250 participants per centre were reached. The study protocol was approved by the Regional Committee for Medical Research Ethics in Norway (REK 2011/1087). Local ethics approval was also obtained in all participating countries. The study was conducted in accordance with the principles of the Declaration of Helsinki.
All patients participating in the study met the following inclusion criteria: age ≥ 18 years; able to read and write in the local language; no severe psychosis. Subjects provided signed informed consent and were examined for dermatological and other physical conditions. Further details of the study have been published elsewhere (4). Out of a total of 3,635 dermatological patients recruited, 682 (18.8%) had psoriasis and were included in the current study for a separate analysis. The group had a mean age of 47.0 ± 15.6 years and 54.2% were male. All patients completed a questionnaire regarding socio-demographic information, negative life events and suicidal ideation. Whenever itch was reported, its severity was assessed using a visual analogue scale (VAS) and subsequently categorized as mild (> 0 and < 3 points), moderate (≥ 3 and < 7 points), severe (≥ 7 and < 9 points) and very severe pruritus (≥ 9 points) (14, 15). Anxiety and depression were assessed with the Hospital Anxiety and Depression Scale (HADS), on which a higher score means a higher level of anxiety or depression (16), and HRQoL was assessed with the Dermatology Life Quality Index (DLQI) (a skin-specific QoL measure) (17) and the EuroQoL (EQ-5D, a generic QoL measure) (18). All instruments were validated in the native languages of participating countries. According to HADS anxiety/depression were considered as unlikely, possible and probable, if a patient received < 7 points, 8–10 points and > 10 points in each subscale, respectively. The DLQI is a 10-item QoL scale assessing “symptoms and feelings”, impairment of “daily activities”, “leisure”, “work and school” and “personal relationships”, as well as “treatment” burden with respect to skin diseases; a higher DLQI score signifies higher impairment of HRQoL (17). Using the EQ-5D, the respondent was asked to indicate his/her general health status indicating the most appropriate statement in each of the 5 predefined dimensions, and answers were converted into scores, with a higher score referring to a higher disease burden. In addition, each participant recorded their self-rated health status with the EQ-5D VAS, where the endpoints were “Best imaginable health state” (0 points) and “Worst imaginable health state” (100 points) (18). Patients were also asked about their satisfaction with their dermatologist (from 0 to 10) and whether they were having or had had suicidal thoughts in the past (yes/no). If they confirmed the presence of suicidal thoughts they were also asked whether their suicidal thoughts were because of their skin condition (yes/no). Finally, skin disease severity was assessed by the dermatologist using a scale of “mild, “moderate” or “severe”.
The results were analysed using Statistica® and Microsoft Excel® software. Frequencies (percentage values) were calculated for qualitative parameters, while means and standard deviations were calculated for normally distributed quantitative variables. The χ2 test, Student’s t-test, multiple regression analysis, analysis of variance (ANOVA) and Pearson’s correlation test were used, where appropriate. Statistical significance level was set at 0.05.
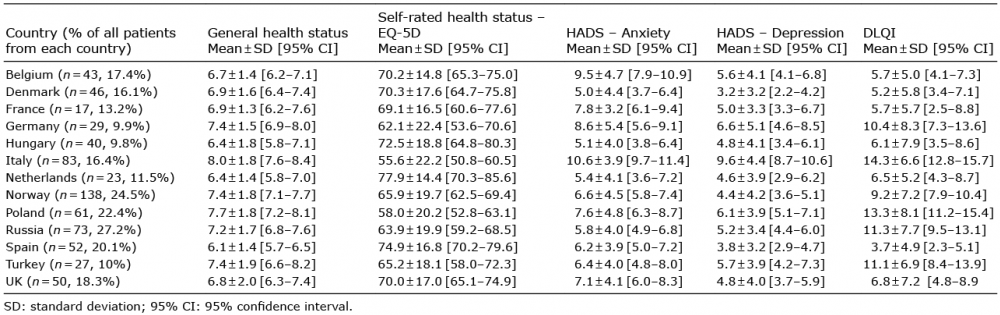
A total of 151 psoriatic patients (22.1%) had HADS-A scoring ≥ 11 points (indicating clinically relevant anxiety) and 91 patients (13.3%) recorded marked depressive symptoms (≥ 11 points). Significant differences regarding self-assessed overall health status, HRQoL, anxiety and depression were observed among psoriatic patients from various European countries (Table I).
Table I. EuroQoL (EQ-5D), Hospital Anxiety and Depression Scale (HADS) and Dermatology Life Quality Index (DLQI) scoring for psoriatic patients from various European countries
The lowest anxiety and depression values were scored by patients from Denmark (HADS-anxiety: 5.0 ± 4.4 points, HADS-depression: 3.2 ± 3.2 points); and the best HRQoL was observed in subjects from the Netherlands (overall health status: 77.9 ± 14.4%; DLQI: 6.5 ± 5.2 points) and Spain (overall health status: 74.9 ± 16.8%; DLQI: 3.7 ± 4.9 points), while patients from Italy were the most impaired (HADS-anxiety: 10.6 ± 3.9 points, HADS-depression: 9.6 ± 4.4 points, overall health status: 55.6 ± 22.2%, DLQI: 14.3 ± 6.6) (Fig. 1). Detailed data on anxiety and depression in particular countries are shown in Table SI.
Fig. 1. Values obtained in different countries. (A) Own health status assessed with EuroQoL (EQ-5D) (red: feeling of poor health, orange: feeling of moderate health; yellow: feeling of quite good health, green: feeling of good health). (B) Anxiety level assessed with Hospital Anxiety and Depression Scale (HADS-A) anxiety subscale (green: anxiety unlikely, orange: suspected anxiety, red: clinically relevant anxiety). (C) Depressive symptoms assessed with the HADS-D depression subscale (green: depression unlikely, orange: suspected depression, red: clinically relevant depression). (D) Quality of life (QoL) assessed with Dermatology Life Quality Index (DLQI) (grass green: normal QoL, green: slightly impaired QoL, yellow: moderately impaired QoL, orange: severely impaired QoL, red: extremely impaired QoL).
Analysis of demographic and socio-economic factors revealed significant correlation between age and general health status assessed with EQ-5D, indicating that higher age was associated with poorer general quality of life (EQ-questionnaire r = 0.15, p < 0.001 and EQ-VAS r = –0.12, p = 0.002), and between age and HRQoL impairment measured with DLQI (similarly, higher age was linked with more decreased HRQoL, r = –0.11, p = 0.005). Also, there was significant correlation, albeit weak, between patients’ age and satisfaction with their dermatologist, indicating that older people are more satisfied with their treating physicians (r = 0.12, p = 0.003) (Table II).
Table II. Relationships between demographic data and patients’ psychosocial well-being
Statistically significant differences between males and females were demonstrated in all analysed aspects, except satisfaction with their dermatologists. Females presented lower overall health status, more intense anxiety and depression symptoms, greater HRQoL impairment and more intense itch compared with males (Table II).
The degree of satisfaction with a dermatologist was inversely proportional to the level of education. There was a low level of anxiety in patients with lower educational attainment, and a high level of anxiety in those with higher educational attainment (Table II).
There were no statistically significant relationships between level of education and severity of pruritus (p = 0.23), overall health status (p = 0.19, p = 0.21), severity of depressive symptoms (p = 0.4) and HRQoL (p = 0.12). Marital status was significantly linked with itch intensity, general health status (EQ-5D questionnaire) and severity of anxiety and depressive symptoms. Divorced people reported more intense itch, higher overall health status impairment, higher anxiety level and more severe depressive symptoms. There were no statistically significant differences between marital status regarding satisfaction with a dermatologist (p = 0.13), self-rated health status (EQ-5D VAS) (p = 0.13) and QoL (p = 0.22) (Table II).
Patients with the lowest socio-economic status (status self-assessed by the respondent as low, middle, or high) demonstrated the highest overall health status impairment, had more severe anxiety and depressive symptoms and the highest HRQoL impairment (Table II).
Disease severity was weakly related to patient’s psychosocial health status, documenting that higher disease severity was linked with poorer well-being. The closest relationship was with DLQI score (r = 0.21, p < 0.001), followed by EQ-5D score (r = 0.18, p < 0.001), EQ-5D VAS (r = –0.17, p < 0.001), depression (r = 0.14, p < 0.001), and anxiety (r=0.1, p < <0.001). A detailed multiple regression analysis on the studied variables influencing the patient well-being is presented in Table SII.
A total of 115 patients out of 668 (17.2%) reported present or past suicidal ideations; out of these patients, 77 (11.5%) stated such ideations to be related to their psoriasis. These patients were characterized by significantly higher severity of pruritus, lower overall health status, more severe anxiety and depressive symptoms, and lower HRQoL compared with patients without suicidal ideation (Table III). The highest prevalence of suicidal thoughts was found in Turkey (44.4%), the lowest in France (5.9%) and the second lowest in Denmark (9.1%) (p = 0.02).
Table III. Relationships between suicidal ideation and psychosocial well-being of psoriatic patients
Multiple regression analysis revealed that the presence of suicidal thoughts was independently related to patients’ age (β = –0.1, p < 0.05), socio-economic level (β = –0.09, < 0.05), stressful life events during the last 6 months (β = –0.18, p < 0.001), general health status according to EQ-5D questionnaire (β = 0.12, p = 0.04), and anxiety level (β = 0.25, p < 0.001), while suicidal ideation related to skin condition were significantly dependent only on stressful life events during the last 6 months (β = –0.1, p < 0.05), and anxiety level (β = 0.24, p < 0.001).
A total of 474 psoriatic patients (69.5%) reported itching, of whom 74.7% reported the presence of chronic itch, i.e. lasting longer than 6 weeks. In some countries the prevalence of itch was extremely high (Italy 91.6%, Germany 82.8%, the Netherlands 82.6%) in comparison with some other countries (France 35.3%, UK 52.0%) (p < 0.001). Significant differences were also observed regarding itch intensity, with the highest scores reported among patients from Italy (mean VAS 6.6 ± 1.9 points), UK (mean VAS 5.8 ± 2.3) and Germany (mean VAS 5.7 ± 3.2), and the lowest scores by patients living in Russia (mean VAS 2.5 ± 3.2), Hungary (mean VAS 3.5 ± 3.3) and Spain (mean VAS 3.5 ± 3.3) (p < 0.001). Detailed data on itch severity scoring are demonstrated in Table SIII.
Patients with chronic itch had more severe pruritus than those with acute itch (6.0 ± 2.5 points vs. 5.3 ± 2.4, p < 0.01). They were also more depressed (Table IV).
Table IV. Relationships between itch and psychosocial parameters in psoriatic patients
Patients with itch had lower overall health status and HRQoL as well as significantly more severe anxiety and depressive symptoms compared with patients without itch. There was a statistically significant correlation between the severity of itch and satisfaction with dermatologist, overall health status, severity of anxiety and depression symptoms, and HRQoL (Table IV).
Psoriasis is a common chronic skin condition that can markedly impair patients’ HRQoL (19–21). Many people with psoriasis report decreased self-esteem and problems in establishing relationships with other people (22). However, in our current study using a validated set of questionnaires we have demonstrated significant variations among different European countries of psychosocial health status of patients with psoriasis. It is possible that cultural differences, different access to possible treatments, differences in the organization of healthcare systems, and differences in climate may influence the impact of psoriasis on patient’s well-being. Differences regarding well-being do not correlate with latitude, ambient temperature or sun exposure, or with national prosperity. The percentage of patients with psoriasis recruited in each centre was highest in Russia, Norway and Poland, and lowest in Turkey, Germany and Hungary. Differences in the patient number included in particular centres may limit the validity of results achieved. In this respect, a further limitation of this study is the lack of data on patients’ nationality, in respect of their duration of stay in the country in which they had been recruited into the study. Another limitation of the study is that patients were recruited on random days, which might not ensure proper random sampling, as some types of patients may be seen on certain days of the week.
Analysis of other demographic data revealed statistically significant differences between males and females in all aspects except for satisfaction with the dermatologist. Females, as also reported by other authors (1, 23), presented lower overall health status, more intense anxiety and depression symptoms, greater HRQoL impairment and more intense itch compared with males. In addition, links were demonstrated between satisfaction with a dermatologist and level of education, between marital status and itch intensity, general health status (EQ-5D questionnaire), anxiety and depressive symptoms severity, between socio-economic status and severity of itch, overall health status, severity of anxiety and depressive symptoms and HRQoL impairment (see Table II).
One of the most important aspects of psoriasis is concomitant pruritus. Approximately 72–80% of psoriatic patients may experience pruritus (22, 24) and this symptom may be one of the main factors influencing their HRQoL (25). The present study confirmed that pruritus is very frequent in psoriasis, and that its severity is one of the main parameters affecting psoriatic patients’ well-being throughout different European countries. As shown, pruritus is considered by patients to be the most bothersome symptom of psoriasis, even though the severity of itch appears to be lower than in other pruritic skin conditions (26). Patients with pruritus show more reduced HRQoL compared with those without pruritus, and pruritus intensity correlates with the degree of HRQoL impairment (26). Pruritus may alter sleep quality, which may further contribute to the alteration of psoriatic patients’ well-being. Psoriatic subjects with pruritus also demonstrate more depressive symptoms (27). This finding may, at least in part, explain the link between pruritus and suicidal ideation, as we found a clear link between the intensity of anxiety and depression symptoms in psoriatic individuals and the presence of suicidal ideations.
This study has several limitations. The way in which patients were recruited and the type of dermatology clinical service may have differed between centres. Although the total number of general dermatology patients recruited at each centre was similar, the number of psoriatic patients depended on the sequential inclusion of psoriatic patients within the larger cohort, leading to differences in numbers of psoriatic patients recruited from each centre. Depending on the local system of referral to the clinic, the clinical severity of the psoriasis patients may have differed between centres. Some of the differences in scores between countries may have been caused by cultural differences in answering the questionnaires. Although validated translations of the measures were used in different countries, giving assurance that the meaning of the questions was as close as possible in the different languages, it cannot necessarily be assumed that the scores from the measures can be directly compared between different countries (28), even though this assumption is made in the interpretation of, for example, multinational drug trials (29). This is a difficulty across all patient-reported outcome measurements in medicine and is not confined to dermatology. Furthermore, disease severity was assessed using only 3 severity categories (mild, moderate, severe). The Psoriasis Area and Severity Index (PASI) would probably be more appropriate as it gives more objective data on psoriasis severity and extent, thus not using PASI should be considered as a further limitation. The same refers to measurement of pruritus intensity, as the VAS is assessing only symptom severity, but does not take into account, for example, pruritus extent or number and durations of itch episodes. Thus, performing only one method of assessment of pruritus severity limits the results for itch. According to the guidelines published by the International Forum for the Study of Itch (IFSI) (8) VAS is one of the most widely used pruritus measures and is recommended for use in all clinical trials on itch. Of course, this instrument, as any other, has some limitations, which have been mentioned in the discussion.
Future studies focusing on the influence of pruritus on patient well-being should consider other measurement tools, such as itch questionnaires (30). However, despite the large number of questionnaires used in our study, in order to keep the study as feasible as possible we decided to include only VAS as a measure of pruritus intensity.
In conclusion, significant variations were observed among different European countries regarding the psychosocial health status of patients with psoriasis. Patient selection biases may have partly influenced the results of the present study, and these findings need to be confirmed in future studies; however, this study indicates that results from one country should not simply be transferred to patients living in other countries, as perception of psoriasis and coping with the disease may take place in a completely different ways. The study clearly indicates that psoriasis is significantly linked with depression, anxiety and impairment of QoL. It is essential to include measures of psychosocial morbidity when assessing psoriasis severity and treatment efficacy, because of the substantial role that psychosocial burden plays in patient perception of disease severity, QoL and disease course (2). Such knowledge also requires the prompt implementation of active interventions to detect and treat psychological disturbances early, in order to improve QoL of patients with psoriasis.


 Click to show fullsize
Click to show fullsize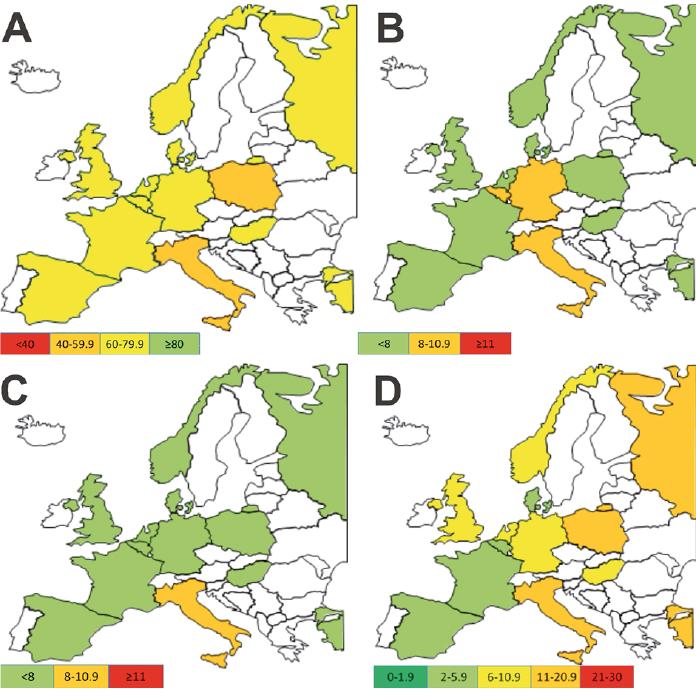 Click to show fullsize
Click to show fullsize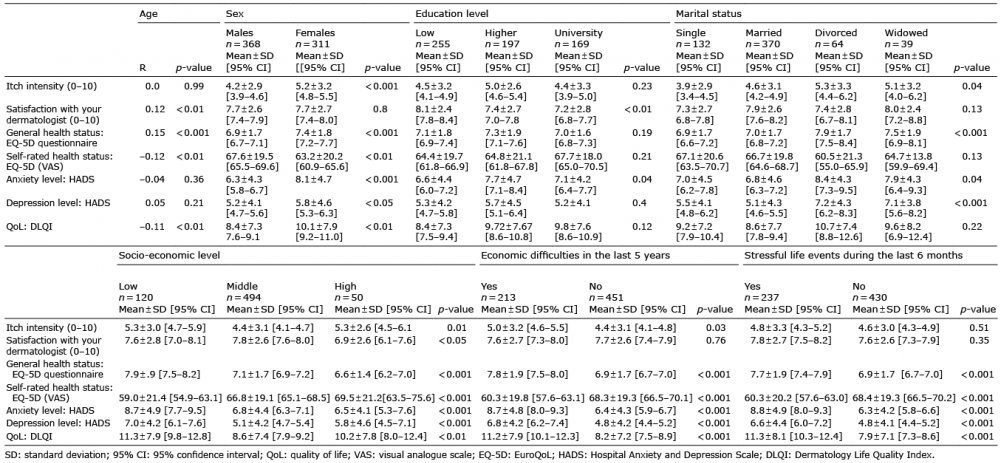 Click to show fullsize
Click to show fullsize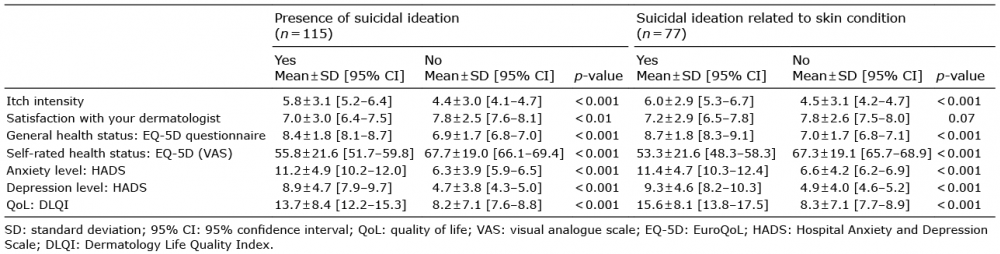 Click to show fullsize
Click to show fullsize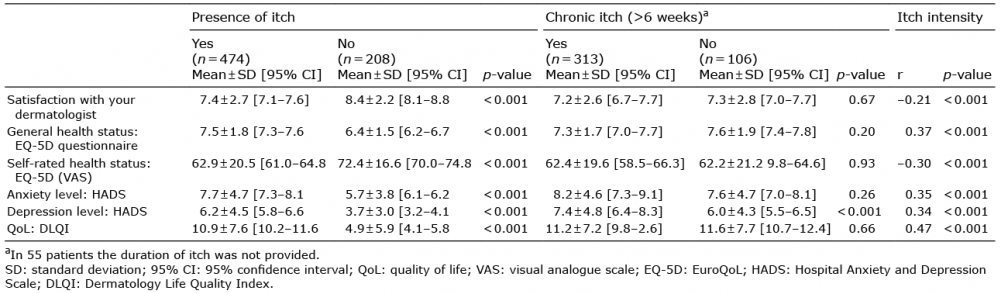 Click to show fullsize
Click to show fullsize